.png)

Gambling harm
What is it, risk factors, presentations, support, and more
"The gambling-related burden of harm appears to be of similar magnitude to harm attributed to major depressive disorder and alcohol misuse and dependence. It is substantially higher than harm attributed to drug dependence disorder.
There is an urgent need to place gambling on national and international public health agendas and strengthen evidence-based policy and prevention strategies, as well as greatly extend early intervention and treatment provision. These measures are critical to reduce current and future harm and social costs associated with commercial gambling."
World Health Organization: The epidemiology and impact of gambling disorder and other gambling-related harm
Author: Dr Kishan Patel, kishan@gamblingharm.com
Contents
What is gambling harm?
Gambling harm can be experienced by people who gamble and by affected others of people who gamble. This refers to people who do not gamble themselves, but experience harm which stems from a person who gambles.
Gambling harm can be notably devastating and can occur over a range of different time modalities.
-
General refers to harm, as the name suggests, which arises from gambling on a general basis, such as the erosion of savings.
-
Crisis refers to harm that is more extreme and has immediate consequences, such as bankruptcy or relationship breakdown.
-
Legacy refers to harms that are experienced over a longer period of time, often which arise out of general or crisis harms, such as ongoing financial hardship or restrictions due to bankruptcy.
Types of gambling harm:
-
financial harm,
-
relationship disruption,
-
conflict or breakdown,
-
emotional or psychological distress,
-
decrements to health,
-
cultural harm,
-
reduced performance at work or study,
-
criminal activity,
-
lifecourse and intergenerational harms
What is gambling disorder?

Gambling disorder (previously pathological gambling) is in the DSM-V and is placed in the ‘Addictions and Related Disorders’ category. It is the only non-substance addiction included.
Gambling disorder is often identified using the DSM-V screen or the PGSI screen.
One way of understanding addiction is through CAGE as both an acronym for signs of addiction (Cut down, Annoyed, Guilty, and Eye-Opener) and a metaphor for how addiction traps the individual and often their loved ones into addiction cycles.
Who does gambling harm affect?
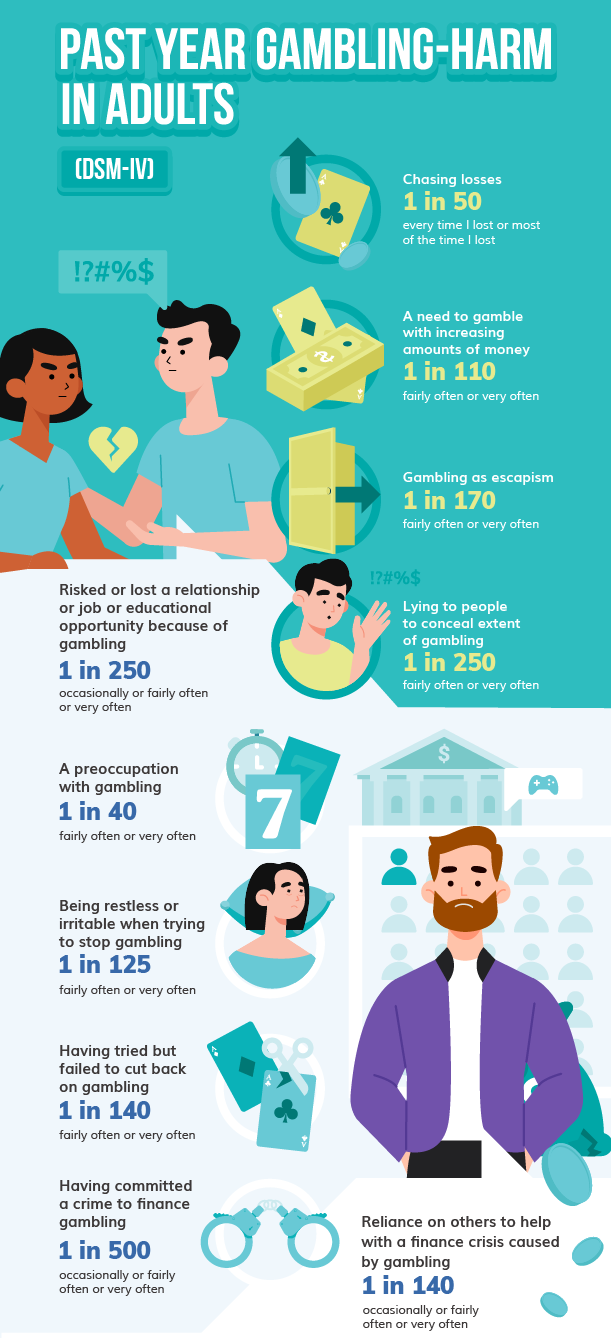
More than 1 in 10 adults in the past year have been significantly affected by gambling harm:
-
8% of adults suffer gambling harm from their own gambling in the past year
-
7% of adults suffer gambling harm from another person's gambling in the past year
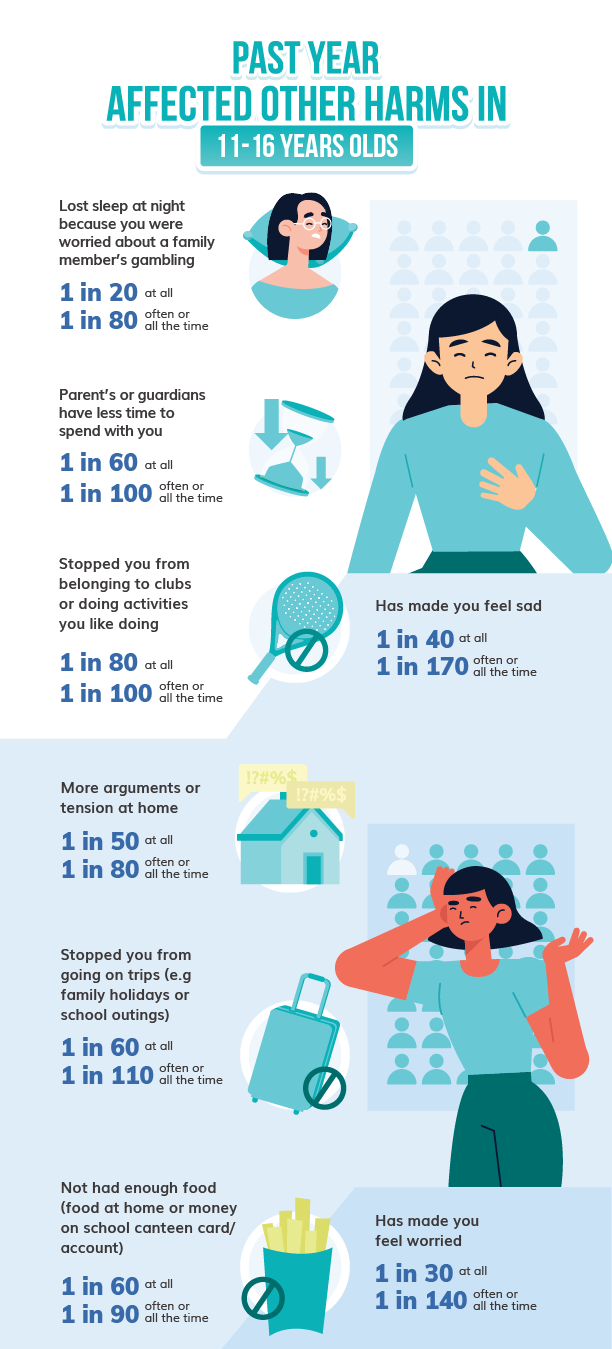
1 in 10 11-16 year olds in the past year have been significantly affected by gambling harm:
-
5% of 11-16 year olds suffer gambling harm from their own gambling in the past year
-
5% of 11-16 year olds suffer negative effects as a results of a family member's gambling in the past year
Research has consistently demonstrated that individuals that are: young, male, and that belong to ethnic minority backgrounds, are disproportionately susceptible to gambling disorder.
It is also important to remember that dopamine agonists, used in Parkinson's Disease and Restless Leg Syndrome, can be an iatrogenic and reversible cause of harmful compulsions to gamble.
Gambling disorder (the most severe level of gambling harm from an individual's own gambling) is between 3 to 5 times more prevalent amongst ethnic minority groups relative to white ethnic groups. Moreover, gambling harm is likely to have a worse impact on those from a minority ethnic background, and this is in part due to differences in cultural attitudes, stigma, and health awareness.
Gambling disorder is also most prevalent amongst 16-24 year olds than in any other age group. In the last gold-standard prevalence survey conducted in Great Britain in 2010, the prevalence of gambling disorder according to the PGSI screen among 16-24 year olds was at 2.0% (males: 2.7%, females 1.2%), whereas the prevalence by PGSI screen of the whole population was measured at 1.0% (males: 1.7%, females 0.3%).

Odds ratios from the British Gambling Prevalence Survey 2010
Parents regularly gambled, but did not have a problem: 1.58, Current cigarette smoker: 2.46, Unmanaged hypertension: 3.19, Unemployed: 4.02, Bad/very bad general health status: 6.17, Parents regularly gambled and did have problems with gambling: 7.32, A low Warwick-Edinburgh Mental Wellbeing score: 7.65
How does the Gambling Industry enable and encourage gambling harm?

Gambling Advertising: The industry maintains that advertising has no effect on consumption but instead helps operators differentiate product offerings and for customers to identify which brands are regulated and therefore can be trusted. Evidence from the Gambling Commission reflects the contrary. Younger adults, in particular, were more likely to be affected by advertising to spend money on gambling when they were not otherwise planning to. Worryingly, this phenomenon has been reported even among 11-16 year olds. The industry is keen to prevent meaningful reform on gambling advertising nationally and internationally because of its importance in driving gambling in the short-term and the long-term through a normalisation effect. The importance of advertising to the industry is highlighted by their lobbying against change and their expenditure.
Design of gambling products: Online gambling has surged over the past decade. With reduced costs and increased accessibility, online gambling is highly profitable to the industry and is unsettlingly addictive for players. Most online games facilitate cognitive biases through the illusion of control and often contain characteristics that particularly appeal to younger customers. The industry has repeatedly resisted reform and suggested that product design has little influence on harm but somewhat down to the individual, despite clear evidence suggesting otherwise.
Online gambling products are subject to:
-
reduced costs,
-
increased accessibility,
-
improved advertisement effectiveness,
-
increased vulnerability to cognitive biases,
-
and increased potential for neurostimulation.
Electronic gaming machines and online casino products have been repeatedly associated with unsettlingly high gambling addiction levels among players. These products have structural characteristics that affect human decision-making and behaviours, and therefore addiction potential, such as:
-
free bet offers,
-
high event frequencies,
-
random ratio reinforcement schedules,
-
near misses,
-
losses appearing as wins,
-
multiline betting, and
-
exaggerated audible and visual reinforcements
Issues with self-exclusion schemes
Self-exclusion schemes can act as a barrier for individuals and prevent them from gambling with either a specific operator or multiple operators across a type of gambling product.
In Great Britain, there are multi-operator self-exclusion schemes for:
-
Online gambling
-
Betting shops
-
Casino
-
Adult Gaming Centres
-
Bingo
Key issues with self-exclusion schemes
-
Awareness: In 2019, 53% of gamblers were not aware of self-exclusion
-
Reliability: Self-exclusion schemes place the onus on the individual to not enter gambling premises and to not gamble. Staff in physical betting shops are often unable to remember faces of individuals signed up to self exclusion schemes in their local area
-
Other barriers to registration: Many self-exclusion schemes are not independent of gambling activity or representation, application forms and instructions may be filled with unnecessary verbosity and complexity, self-exclusion schemes may only be available in English at certain hours of the day (Gamstop for online gambling is an exception to this issue)
How can gambling harm present in the healthcare setting?
Gambling disorder symptoms may be masked by preoccupation and so may present silently or with physical symptoms of withdrawal or poor self-care or low mental wellbeing.
Common symptoms of withdrawal include sweating, clammy skin, anxiety, depression, mood swings, and night sweats.
The case studies below represent real-life accounts of gambling harm where the clinician had not identified the role of gambling in the health issue - because they did not ask.
Presenting complaint in children affected by a family member's gambling
-
2 year old presents at A&E after "falling down the stairs" and hitting their head
Non-accidental injury: Mother and patient suffer domestic abuse associated with gambling harm
-
9 year old presents with father worried about a low BMI
Inadequate nutrition: the patient doesn’t eat much at school, due to payday poverty meaning that there isn't enough money to pay for food and not eligible for free school meals due to parents earnings
-
12 year old presents with chest pain and worries that they might be having a heart attack
Anxiety attacks/familicide: the patient has tried to run away from home a few times, they are scared because their father said that they are ‘ticking time bomb’ and will kill the whole family. The patient doesn’t want to live and has pulled a knife on themselves but were unable to hurt themselves as they were stopped
-
14 year old presents with a complaint of feeling ill all the time
Allergic rhinitis: the patient reports rhinitis symptoms that persist all the time when at home, the home has mould and is cold because there is not enough money to solve the mould issues or keep the house warm
-
15 year old presents with a complaint of feeling tired all the time and is worried it might be something like diabetes
Inadequate sleep/insomnia: the patient finds it difficult to get to sleep and stay awake, they feel like their mind is running with too many thoughts before sleep, and they are worried they may be attacked in the middle of the night
-
18 year old presents with abdominal pain with a patient-reported severity of 8/10 as well as irritable bowel and bladder symptoms
Irritable bowel syndrome/irritable bladder: the patient’s father passed away three years ago and this is when the symptoms started, as well as struggling with bereavement and guilt, the patient studies 5 A-levels and works part-time to help cover their costs in the household as the family has a lot of debt
Presenting complaint in adults affected by gambling disorder
-
28 year old presents with poor glycaemic control on insulin therapy
Poorly controlled diabetes/chronic condition: the patient has difficulty maintaining a healthy lifestyle as well as difficulty with remembering to take their medications due to them working long hours and having a preoccupation with gambling
-
30 year old presents with a 20 pack year history
Current cigarette smoker: the patient wants to cut down and stop but they work long hours and so find it extremely difficult to stop for more than a few months
-
33-year-old presents with poor mental wellbeing and suicidal ideation
Depression/Suicidal Ideation: the patient has been having thoughts about ending their life because they recently lost £10, 000 in a single day and they blame themselves for all the debt that they've accrued through gambling. They are stressed because it will take years to get out of debt
-
52 year old passes away from a myocardial infarction whilst at work
Death at a young age: the coroner reports smoking and diabetes significant, but omits the fact that the patient worked long night-shifts and struggled to cope due to a 20+ year history of an undiagnosed gambling disorder
How can gambling harm affect someone's health?
Gambling harm as Years of Life Lost due to Disability
General:
-
Increased sedentary behaviour during time spent gambling
-
Biological manifestation of emotional and psychological distress eg. increased blood pressure, loss of sleep, loss of sleep, migraine, nausea, diarrhoea
-
Reduced levels of self-care:
-
nutrition
-
hygiene
-
sufficient sleep
-
compliance with medical care
-
physical activity
-
reduced quality of living circumstances (ie. cannot afford heating)
-
-
Incidence of disease or injury due to reduced levels of self care
-
Increased risk due to gateway effect, interaction with, or exacerbation of other health risk factors (drinking, smoking, illegal substances)
-
Increased risk due to gateway to, interaction with, or exacerbation of comorbidities (depression, anxiety, biophysical chronic disease)
-
Increased experience of family violence due to involvement in gambling
-
Incidence of self-harm
-
Increased risk to physical wellbeing of affected other in the care of the person who gambles due to their distraction or tiredness
-
Minor health ailments (headache migraine) relating to focussing on a screen for long periods of time with particular gambling products
-
Physical impacts of other gambling harms: financial, relationship, emotional, cultural, work or study, criminal

Crisis:
-
Onset of health condition due to exacerbation of risk factors or continued stress from other harms
-
Physical impacts of living rough due to homelessness, including increased risk of disease, violence and impact of poor living conditions
-
Experience of violence due to involvement in gambling
-
Medical emergency (including mortality) due to onset, exacerbation, or failure to diagnose condition due to gambling
-
Serious self-harm
-
Attempted (or completed) suicide
Legacy:
-
Ongoing disability or decrement to health through attempted suicide or other forms of self-harm
-
Ongoing increased risk of disease or decrement to health due to legacy effects of risk factors or poor self-care
-
Ongoing disability or decrement to health due to other medical conditions exacerbated or advanced due to involvement with gambling.

Gambling harm as Years of Life Lost due to Mortality (YLL)
-
The last Adult Psychiatry Morbidity Survey 2007 that considered gambling-harm reported that individuals with gambling disorder were more likely to have thoughts about suicide (19.2% vs 4.1%) and to have made a suicidal attempt in the past year (4.7% vs 0.6%) compared to individuals who do not suffer gambling-harm
-
Research from the UK involving bank data from over 100, 000 customers found that high levels of gambling were associated with a 37% increase in mortality
-
Men and Women in Sweden, aged 20-49 year olds and diagnosed with Gambling Disorder, were 19.3 times more likely to suffer from suicide when compared to the general Swedish population of the same ages
-
Men and Women in Sweden, aged 20-49 year old and diagnosed with Gambling Disorder, were 6.2 more likely to suffer from any mortality when compared to the general Swedish population of the same ages
How can gambling harm be managed or treated?
Unfortunately, the UK (NICE) does not currently have any guidelines for the treatment and management of gambling harm. The expected publication of NICE guidelines on gambling is due on 07th February 2024. Instead, health care professionals may want to refer to MONASH University (Australia): Guidelines for Screening, Assessment and Treatment
The National Gambling Helpline gives confidential information, advice and support for anyone affected by gambling problems in England, Scotland and Wales. (24/7 free helpline: 0808 8020 133, or via live chat on www.gamcare.org.uk).
There is also further information and signposting on the NHS Live Well site.
